Childhood Leukemia International Consortium
Dr. Catherine Metayer is the chair of the Childhood Leukemia International Consortium (CLIC, formerly referred to as Project 1 during the first funding cycle of CIRCLE, 2009-2015). As part of CIRCLE, Dr. Metayer worked hard to bring together investigators from many different countries to participate in a unique collaborative effort. CLIC pools information from studies all around the world to answer the big questions in childhood leukemia research.

Alone we can do so little. Together we can do so much
-Helen Keller
Collaboration is Key
Relative to the chronic health problems that plague adults, such as cardiovascular disease and diabetes, childhood leukemia is a relatively rare disease. From an epidemiological perspective, this makes childhood leukemia more challenging to study, because the incidence rate limits the scope of the investigation. Moreover, childhood leukemia is actually a catch-all term for an amalgam of disease subtypes, which are etiologically and clinically distinct; each one having its own set of causes and range of outcomes. In addition, each of the childhood leukemia subtypes is potentially multifactorial, with several circumstances contributing to the initiation of each leukemia case. To account for the complexity of the disease, researchers must consider the cumulative impact of joint exposure to an overwhelming mixture of chemicals as well as the unique genetic susceptibility inherent in each child. Together, these two factors — exposure and genetics — must be considered in the context of the child’s life course, as specific windows of time (such as the prenatal period) may be especially important for disease initiation. All of these challenges — small sample sizes, diverse disease subtypes, and a complex, mutlifactorial disease — make international collaboration in childhood leukemia research essential. When data is pooled across studies, the available sample size increases, enabling investigators to draw more precise conclusions. This type of pooled anaylsis opens the door to stratification by disease subtype, evaluation of gene-environment interactions, and parsing out the effects of exposure at distinct windows of time
Who are the members of the Childhood Leukemia International Consortium?
CLIC is comprised of 32 case-control studies from 21 countries in North and South America, Europe, Africa, and Oceania. Together, these studies have collected valuable research information from the families of ~32, 000 children with leukemia and up to 2.3 million controls. In 2017, the CLIC consortium expanded to other pediatric cancers such as brain tumors (~14,000 children) and non-central nervous system embryonal tumors (~14,000 children).
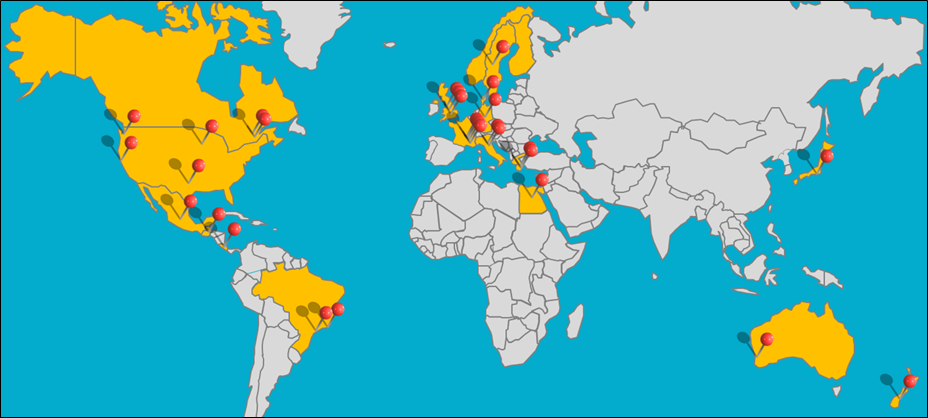
Map of Studies Participating in the Childhood Leukemia International Consortium
Initial Findings of Childhood Leukemia International Consortium
CLIC has identified – with enhanced precision – associations of childhood leukemia with multiple chemicals, immune factors, prenatal folic acid/vitamin supplementation, and fetal growth. Analyses have evaluated these environmental risk factors alone and in combination with genetic factors, on childhood leukemia risk overall and by subtype. Pooled analyses were conducted using information about ~9,000 children with acute lymphoblastic leukemia (ALL), 1,300 children with acute myeloid leukemia (AML), and 15,000 healthy control children from 14 studies. References to CLIC publications can be found on the Resources page.
- CLIC strengthened the evidence of modest associations between paternal ever-smoking and childhood AML, with dose-response relationships. Elevated risks were seen for maternal smoking during pregnancy only among Latino women.
- Home paint exposure shortly before conception, during pregnancy, and/or after birth was associated with an increased risk of childhood ALL and AML. Risks were greater for professional painting and specific cytogenetic subtypes of childhood leukemia.
- Home pesticide use before and/or after birth was associated with an increased risk of childhood ALL overall; elevated risks were observed for most subtypes and with most types of pesticides. An elevated risk of AML was reported for prenatal exposure only.
- Paternal preconception exposure to pesticides at work was associated with increased ALL risk, whereas no association was seen with maternal occupational exposure during pregnancy. In contrast for AML, an association with maternal exposure during pregnancy was observed and no association was seen for preconception paternal exposure.
- Children born by pre-labor caesarean delivery were found to be at an increased risk for developing ALL relative to children who were born by vaginal delivery.
- Reduced risks of childhood ALL and AML were associated with maternal intake of folic acid and vitamins before and during pregnancy.
- Pooled analyses supported the hypothesis that child’s immune status and fetal growth are pivotal pathways in the etiology of ALL.
- Two pooled analyses showed that high coffee intake during pregnancy may increase the risk of childhood acute lymphoblastic and myeloid leukemias.